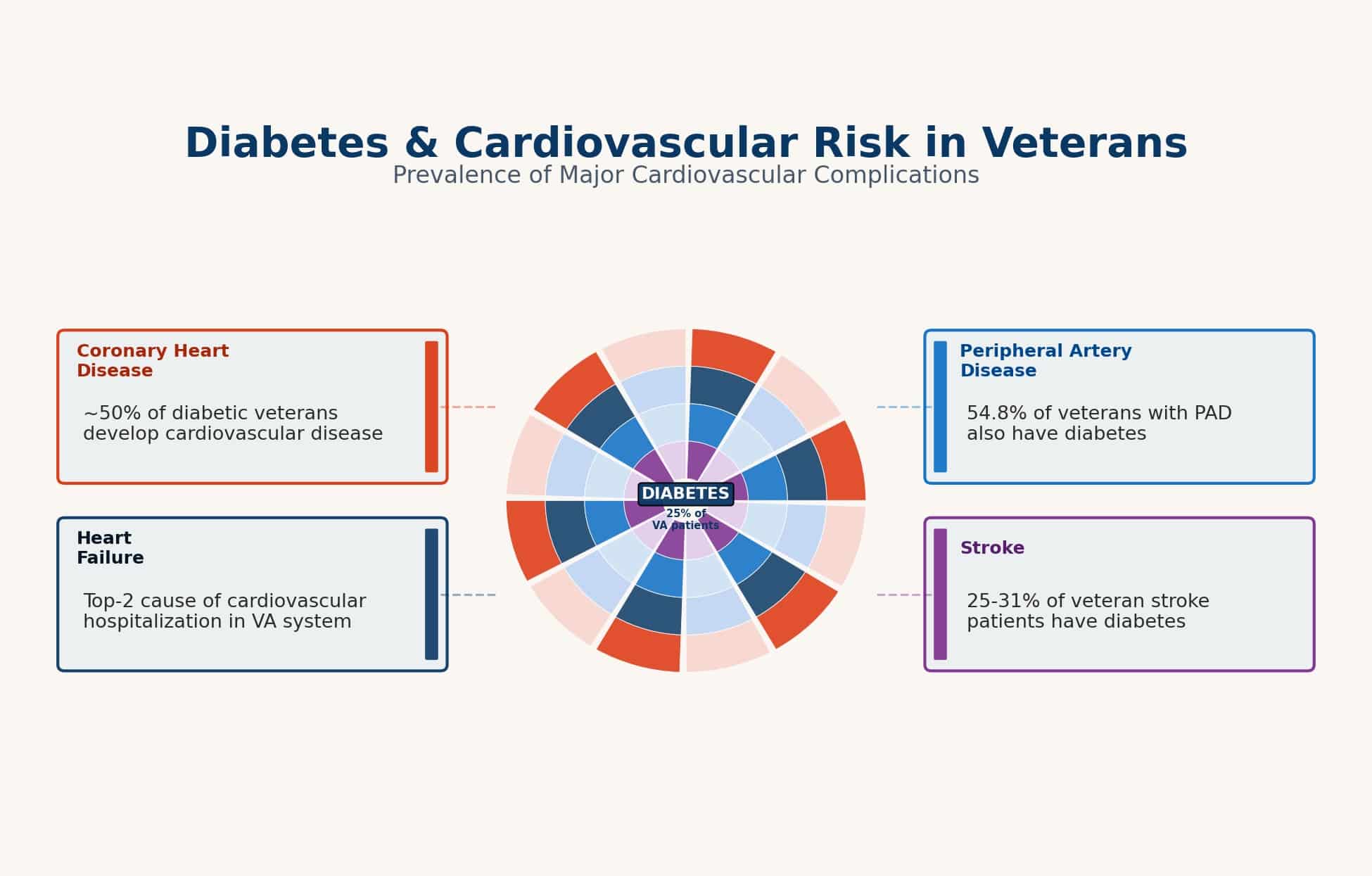
Diabetes has long been associated with damage to the heart and blood vessels. Research shows that by the time the condition is identified, veterans with diabetes have a higher risk of heart disease than the general population. This can include conditions such as coronary artery disease, congestive heart failure, diabetic cardiomyopathy, and others.
However, heart disease secondary to diabetes is one of the most complicated claims to prove, because these two conditions rarely come alone. They’re usually part of a bigger picture called metabolic syndrome: belly fat, high blood pressure, high blood sugar, high triglycerides, and low HDL cholesterol.
These fuel each other and untangling which one caused which is something even doctors debate. Did diabetes damage the heart? Did high blood pressure make everything worse? Often the answer is all of the above. Because of this complexity, you need more than a standard VA exam in your claim file.
We explain how the VA evaluates claims of heart disease secondary to diabetes, what evidence helps prove the connection, and how you can pursue the highest rating (up to 100%) available for all your disabilities.
Heart Conditions That Can Be Claimed as Secondary to Diabetes
Persistent insulin resistance can lead to atherosclerosis, which is the leading cause of cardiovascular risks from diabetes. Atherosclerosis involves stiff, narrow blood vessels and reduced blood flow, often causing or worsening cardiovascular conditions such as:
- Coronary Artery Disease (CAD) – a dangerous form of atherosclerosis that occurs in the large vessels of the heart
- Hypertension – increased blood pressure from narrow/stiff arteries, making it harder for blood to flow. Hypertension is not evaluated as a heart disease; the VA rates it separately.
- Ischemic cardiomyopathy – weakening, stiffening, and enlargement of the heart due to atherosclerotic plaque buildup, caused by reduced oxygen levels
- Congestive heart failure (CHF) – inefficient pumping of the heart from reduced oxygen-rich blood to the heart muscle
- Cerebrovascular accident (stroke) or myocardial infarction (heart attack) – an interruption of blood flow to the brain (ischemic) or bleeding in the brain (hemorrhagic), which can cause lasting effects
Diabetes complications such as chronic inflammation or neuropathy can also cause or worsen heart disease in veterans with diabetes:
- Cardiomyopathy - structural and/or functional heart muscle damage resulting from chronic high blood sugar, insulin resistance, and dyslipidemia (high lipid levels, such as cholesterol)
- Cardiac arrhythmias – abnormal heart rhythms from autonomic neuropathy (damage to nerves that control the heart rhythm, caused by chronic high blood sugar)
- Cardiac Autonomic Neuropathy (CAN) – damage to nerves that regulate heart rate, leading to severe cardiovascular problems like arrhythmias and other myocardial ischemia or orthostatic hypotension (drop in blood pressure when standing)
How to Win a Secondary VA Disability Claim
To establish secondary heart disease, veterans must meet VA requirements by presenting the correct legal basis for the claim and providing specific documentation.
Secondary Connection Requirements
- Current diagnosis of the heart/cardiovascular condition (e.g., CAD, cardiomyopathy, CHF, arrhythmia, hypertension).
- Service-connected diabetes (you can file a claim for the heart condition while diabetes is still pending, but secondary connection generally can’t be granted until the diabetes is service connected).
- A medical nexus opinion stating diabetes caused the heart condition or aggravated it beyond its natural progression, with an explanation tied to the veteran’s records.
Secondary service connection is established under 38 C.F.R. § 3.310. Once it’s granted, VA rates the heart disease from 10% to 100% under 38 C.F.R. Part 4 (§ 4.104 for most heart and vascular conditions). The VA looks for:
- Supporting diagnostic or laboratory medicine/pathology tests (stress test, echocardiogram, cath / angiogram, EKG, CT scans, etc.)
- Treatment evidence (hospitalizations, treatments such as medications, stents, CABG, implanted devices such as pacemaker / AICD, etc.)
The VA commonly relies on objective measures such as METs capacity, ejection fraction (EF), documented episodes of heart failure, specific treatments or hospitalizations. Submitting the actual test reports (not just summaries) helps VA rate the disability accurately.
Building a Timeline
Without a timeline of the disease process and symptoms, the VA may claim that the heart condition occurred before diabetes, or that heart disease is completely explained by genetics or by other factors, such as obesity or smoking. Follow the chronological order:
- Diabetes diagnosis – including the date of the initial diagnosis and current medical records that show the condition is ongoing and actively managed
- Heart disease diagnosis – including the original date of diagnosis (which is optimally after the diabetes diagnosis)
- Worsening disease/symptoms course – consistent with diabetic vascular or heart disease
If the heart condition existed before diabetes (or before diabetes was diagnosed), VA often looks for evidence of a baseline level of severity and objective proof that diabetes worsened the condition beyond its normal course.
Helpful indicators include increasing medication requirements, worsening blood pressure control, declining ejection fraction (EF), reduced METs capacity, more frequent ER visits/hospitalizations, or earlier need for procedures (stents/CABG).
The Nexus Opinion
In a VA disability claim, a nexus is the link (direct or indirect) between a disability and military service. It’s often supported by a nexus letter, written by a qualifying, licensed provider. A strong nexus opinion for heart disease secondary to diabetes should include:
- Language stating that heart disease is “at least as likely as not” (50% or greater probability) caused by or aggravated by service-connected diabetes (recognized by the VA to have been caused or aggravated by the veteran’s military service).
- Explanation of how the veteran’s diabetes accelerated atherosclerosis, endothelial dysfunction, microvascular disease, etc.
- Documentation regarding other, competing risks such as family history, smoking, or etiologies (other conditions) such as obesity, high blood pressure (hypertension), high lipid levels (cholesterol, etc.)
For faster claims approval, ask your provider to state that your heart condition was either caused by diabetes or that there was at least a 50% chance your diabetes accelerated the progression of heart disease. Including both explanations gives the VA multiple paths to approve your claim.
Paths to Claiming a Heart Condition Secondary to Diabetes
1. Heart Disease Directly Caused by Diabetes
This pathway shows the heart condition developed over time as a direct result of diabetes-related damage. Long-term high blood sugar levels harm blood vessels and trigger inflammation, leading to secondary cardiovascular conditions.
Example: Diabetic Cardiomyopathy
A provider may explain that long-term diabetes-induced metabolic changes directly led to functional and structural damage to the heart without evidence of atherosclerosis (confirmed by medical/lab and imaging tests).
Example: Coronary Artery Disease
Diabetes injures the heart’s arterial lining and promotes plaque buildup (atherosclerosis), restricting blood flow. A medical opinion should state that the CAD is at least as likely as not the result of long-term, uncontrolled diabetes.
2. Worsening of an Existing Cardiac Condition
This pathway applies when a heart condition already existed but was not severe enough to qualify for its own rating (or may have received a low rating), and diabetes worsened the condition. The focus is on showing the condition progressed beyond what would usually be expected.
Example: Accelerated Atherosclerotic Disease
Diabetes increases the rate of arterial plaque buildup, without other risk factors (such as family history or other cardiovascular conditions), which may lead to earlier onset and more severe symptoms and outcomes (like a heart attack) sooner than it would usually be expected.
Getting Separate Ratings for Complications
Diabetic complications include physical damage caused by the natural progression of the disease to blood vessels, nerves, and other structures. Complications are diabetes-related medical problems, while secondary conditions are how the VA recognizes and rates conditions that arise from complications.
Complications from diabetes are often rated as separate conditions, depending on various factors such as when they:
- Have a formal diagnosis
- Are service connected
- Are distinct from core diabetes symptoms
- Have documentation focused on conditions such as diabetic neuropathy, diabetic retinopathy, or heart disease
If a complication does not qualify for its own rating (noncompensable), the VA may treat it as part of the overall diabetic condition. This can be used to support higher disability compensation for diabetes.
How Are Complications Evaluated and Compensated?
- Noncompensable complications: early or mild changes from diabetes, such as minor vision changes, that are not severe enough for their own rating and are included within the main diabetes evaluation
- Compensable complications: more serious conditions stemming directly from diabetes, such as peripheral neuropathy, diabetic retinopathy or kidney disease, qualify for separate ratings
- Secondary service-connected conditions: these include cardiovascular problems, which are evaluated separately from diabetes and rated under heart-specific criteria (DC 7005–7015)
Coronary Artery Disease Secondary to Diabetes
Veterans need to show medical evidence of the secondary condition diagnosis and how diabetes contributed to the condition. A strong nexus (medical connection) explaining how the condition is linked with military service is also required.
Supporting Evidence
- A recent diagnosis from a cardiologist – describing coronary artery disease (CAD), ischemic heart disease, or atherosclerosis (plaque buildup in the arteries)
- Cardiac catheterization or coronary angiography results – showing stenosis (narrowing of the arteries), or a history of stent placement or coronary artery bypass grafting (CABG), a procedure that reroutes blood flow around blocked arteries.
- Stress test results – showing reduced heart function or blood flow problems
- Imaging test results – such as a CT coronary calcium scan (test that measures calcium buildup in arteries, signaling plaque and blockage risk)
The provider must explain how the CAD is medically linked to the veteran’s diabetes to establish the nexus. This is accomplished by using clinical reasoning and showing a clear timeline. A strong medical nexus includes:
- A detailed explanation that diabetes mellitus expedited plaque buildup and harmed the inner lining of blood vessels (endothelial dysfunction, meaning the vessels cannot function normally)
- A timeline showing that diabetes was developed/diagnosed first or that it worsened CAD, expediting the need for heart disease procedures or ongoing treatment
- A balanced review of other risk factors (high lipid levels, smoking, or family history), while explaining how diabetes was the prime factor that played a significant contributing role.
Cardiomyopathy Secondary to Diabetes
Diabetes can lead to a distinct type of heart disease called diabetic cardiomyopathy that is not caused by blocked arteries (like in CAD), but rather, occurs from damage to the heart muscle, from chronic high blood sugar.
CAD and cardiomyopathy can occur together, and diabetes increases the incidence of both conditions. CAD can also lead to heart failure (a condition where the heart cannot pump enough blood to meet the body’s needs).
Winning a Cardiomyopathy VA Claim
A winning cardiomyopathy VA claim often depends on whether the cardiologist provides a compelling medical explanation of how diabetes either caused the cardiomyopathy or worsened it (beyond its usual course) compared to other possible etiologies (causes).
Supporting Evidence
An echocardiogram is an ultrasound to evaluate the heart’s structure and function (including how efficiently the heart pumps). It can show, for instance:
- Dilated cardiomyopathy – the most common form of cardiomyopathy, involving weakening of the heart chambers that reduces its pumping strength
- Hypertrophic changes – thickening of the heart muscle that limits proper filling and blood flow
- Diastolic dysfunction – impaired relaxation of the heart between beats, which causes improper filling of the heart chamber
- Ejection fraction (EF) - a measurement of ventricular ejection (how much blood is pushed out when the lower left chamber contracts)
A cardiac MRI can reveal structural and functional changes that may not be detected by standard tests. Evidence provided by a cardiac MRI may be key to supporting a VA disability claim for diabetic cardiomyopathy.
If the condition is non-ischemic (not caused by blocked arteries), your clinician should review other possible causes and explain why diabetes is “at least as likely as not” a major contributing factor in cardiomyopathy, or worsens it beyond its normal progression.
If significant artery blockage is present, the VA may classify the condition as ischemic cardiomyopathy. This still supports your claim as you can link coronary artery disease to diabetes, then cardiomyopathy as secondary to CAD.
Congestive Heart Failure Secondary to Diabetes
Congestive heart failure (CHF) occurs when the heart cannot pump effectively. Diabetes Mellitus (type 2 diabetes) increases the risk of CHF by damaging both the blood vessels and the heart muscle. Often, CHF develops slowly, over time, as other heart conditions (such as coronary artery disease, high blood pressure, and cardiomyopathy) worsen.
A comorbid condition is the simultaneous presence of two or more medical conditions. Common comorbid progression pathways in CHF include:
Diabetes → CAD → CHF
Diabetes contributes to coronary artery disease by causing plaque buildup that narrows arteries, reducing blood flow to the heart. Over time, this strain weakens the heart muscle, leading to CHF. The VA refers to this as “a chain secondary connection”.
Diabetes → Cardiomyopathy → CHF
Diabetes can directly damage the heart muscle (diabetic cardiomyopathy). This leads to stiffness of the heart muscle or reduced pumping ability, eventually progressing to heart failure, particularly with a decline in ejection fraction (the amount of blood pumped out with each heart contraction).
Evidence for Secondary Congestive Heart Failure Claims
VA evaluators look for certain test results and medical documentation for a winning CHF disability claim, including:
- A recent CHF diagnosis by a cardiologist
- An echocardiogram (heart ultrasound) – showing reduced EF, diastolic dysfunction (impaired relaxation or increased stiffness of the heart muscle), or heart chamber enlargement
- BNP testing – a blood marker that increases when the heart is under stress
- Records of hospital admissions or use of diuretics – a cornerstone treatment of CHF involving medication to remove excess body fluid
- METs testing – measuring how well the heart performs during physical activity
Supporting Medical Notes and Opinions
- A definitive medical statement explaining that diabetes increased the severity and frequency of heart failure episodes
- Medical documentation explaining how diabetes worsens heart muscle performance (myocardial function), contributes to damage of small blood vessels (microvascular disease), and causes changes in how the heart uses energy (metabolic remodeling).
- A medical opinion focusing on how the primary condition aggravated CHF when CHF occurred before the primary/contributing condition (such as CAD or cardiomyopathy), by showing more hospitalizations, higher medication needs, or a decline in EF over time
Cardiac Arrhythmia Secondary to Diabetes
Cardiac arrhythmias are abnormal heart rhythms causing the heart to beat too fast (tachycardia), too slow (bradycardia), or irregularly due to problems with its electrical system. Rather than a standalone condition, arrhythmias are often a complication of underlying heart disease.
Cardiac arrhythmias caused by coronary artery disease may receive a separate VA rating when classified as “persistent” (such as in ventricular rhythm disorders) or when treatment involves a long-term pacemaker or an implantable cardioverter defibrillator (AICD).
There are several key pathways to establish service connection for arrhythmias, including:
Diabetes → CAD → Arrhythmia
Diabetes contributes to CAD’s arterial narrowing from plaque buildup, which can cause scar tissue in the heart and reduce blood flow. This damage disrupts the heart’s electrical signals, leading to arrhythmias, particularly in areas affected by ischemia (reduced oxygen supply).
Diabetes → Cardiomyopathy / CHF → Arrhythmia
Diabetes can weaken or stiffen the heart muscle, such as in cardiomyopathy, leading to congestive heart failure (from reduced pumping ability). These conditions increase the risk of atrial (upper heart chambers) fibrillation (AFib) or ventricular arrhythmias (VFib).
Diabetes Aggravates Arrhythmia
In some cases, diabetes may worsen an existing rhythm disorder. This scenario applies when consistent low blood sugar levels occur during arrhythmia episodes or with autonomic dysfunction (damage to the nerves that control heart rate).
Evidence to Support a Secondary Cardiac Arrhythmia Claim
- An electrocardiogram (EKG): tests that records heart rhythm, showing various types of arrhythmias, including atrial fibrillation (AFib), a rapid rhythm from upper chambers called supraventricular tachycardia (SVT), a fast rhythm from lower chambers (ventricular tachycardia), or frequent premature ventricular contractions (PVCs, extra beats)
- A Holter monitor report: a portable device that tracks heart rhythm over time and during resting periods and activities
- Electrophysiology reports: detailed findings of a specialized procedure that records the heart’s electrical system to diagnose and treat cardiac arrhythmias
- Cardiology notes: medical documentation linking heart rhythm problems to structural heart disease
- Implanted device records: from a pacemaker or an implantable cardioverter-defibrillator
If the VA attempts to separate arrhythmia from the conditions that contributed to it, the medical opinion should explain that the irregular heart rhythm is a predictable complication of the service-connected CAD, CHF, or cardiomyopathy, caused by diabetes.
Other VA Conditions Secondary to Diabetes
Veterans already service-connected for diabetes who are pursuing a secondary rating for heart disease may increase their overall combined rating by requesting that the VA also evaluate and rate diabetic conditions from complications such as neuropathy, eye disorders, and other associated medical conditions. These can sometimes affect the veteran’s health in a way that also contributes to heart disease.
Peripheral Arterial Disease and Peripheral Vascular Disease
Peripheral artery disease (PAD) is a circulation disorder in which narrowed arteries limit blood flow to the limbs (usually in the legs). PAD develops when fatty deposits build up along arterial walls outside of the heart, causing them to stiffen and restrict blood flow.
For VA disability purposes, PAD and PVD are rated as distinct conditions under 38 CFR § 4.104, separate from heart disease ratings. If diagnosed, they can be evaluated on their own, even when linked as secondary to diabetes or ischemic heart disease or diabetes.
This allows the VA to account for broader vascular damage throughout the body (which increases the risk of heart attack and stroke), strengthening the heart disease claim.
For PAD, leg pain (claudication) is a limiting factor rather than shortness of breath (as in a CAD claim). Mobility loss and activity restrictions become more severe when both CAD and PAD occur, because exertion is at its peak level.
Stroke and Residuals
Diabetes and vascular disease often occur alongside CAD and hypertension, increasing the risk of stroke. In VA disability claims, the focus is not just on the stroke itself but on the lasting residual effects that remain after the stroke occurs. Stroke residuals include:
- Weakness or coordination problems – challenges using one side of the body or performing fine motor tasks
- Speech or swallowing difficulty – trouble speaking clearly or safely eating due to a choking hazard from damage to the muscles or nerves involved in swallowing
- Cognitive or executive dysfunction – reduced ability to plan, think, or make decisions
- Balance problems and fatigue – unsteady movement and chronic low energy, limiting daily activity
These impairments often significantly impact a veteran’s ability to work and live independently. When stroke residuals are combined with heart conditions like CAD or CHF, particularly with physical exertion limitations, the overall impact can be severe.
Diabetic Kidney Disease
Diabetic kidney disease (DKD), also called diabetic nephropathy, occurs when chronically elevated blood sugar levels damage the kidneys. As kidney function worsens, related conditions (such as heart disease) also become harder to control.
Diabetes, kidney disease, and CAD/CHF are often intertwined (each disorder worsening the other’s symptoms) and result in:
- Systemic damage and heart function decline – kidney injury affects blood vessels throughout the body, which can worsen CAD or CHF and create a harmful cycle between heart and kidney function
- Worsening secondary conditions – declining kidney function leads to edema (fluid buildup), increasing swelling, and worsening heart failure symptoms
- Blood pressure control issues - as kidney function worsens, hypertension becomes more difficult to manage, further accelerating both kidney and cardiovascular damage
- The need for medication adjustments – reduced kidney function often affects optimal absorption of medications, requiring close monitoring of drugs such as antihypertensives (high blood pressure drugs)
Peripheral Neuropathy in Legs and Sometimes Arms
Diabetic peripheral neuropathy is a type of nerve damage (usually involving the feet and legs), caused by chronic high blood sugar levels. Symptoms include a burning sensation, tingling, weakness, numbness, and pain in the extremities. The condition can lead to severe injuries (such as falls due to numbness) or foot ulcers.
Neuropathy can affect the functional aspect of heart disease by reducing safe activity and exercise, necessary to help keep heart disease in check. A veteran who may otherwise tolerate physical exertion may no longer be able to sustain it without risk.
Neuropathy is rated similar to sciatic nerve paralysis (DC 8520) for the lower extremities or under related codes for neuritis (nerve inflammation), DC 8620, and neuralgia (nerve pain), DC 8720. See the VA ratings for diabetic neuropathy.
Diabetic Eye Disease
Eye disorders, such as diabetic retinopathy or macular edema, are common secondary conditions for diabetes and their functional impact often includes:
- Increased fall risk: blurred vision or other visual impairments increase the risk of falls, particularly in those with heart disease symptoms such as dizziness
- Limited ability to drive – reduced vision can prevent safe travel to medical visits or other appointments
- Difficulty managing self-care – vision impairment often interferes with the ability to read medication labels, follow medical instructions, or use monitoring devices, as well as inhibiting the ability to perform proper heart or diabetic self-care
The VA may assign a separate rating for eye conditions, and when combined with heart-related limitations, it often shows a more complete picture of how these issues affect everyday functioning and employability.
If you are a veteran with diabetes trying to get rated for heart disease and other complications but your claim has been denied, get in touch with us for a free, no obligation case review. Hill & Ponton lawyers specialize in winning complex cases, such as diabetes with secondary conditions and multiple complications, with no upfront costs.
Maximize Your Benefits
Unhappy with your VA decision? We’re here to help. Contact us for a free review of your case.
Content Reviewed by
Shannon was born on MacDill AFB in Tampa, Florida as the daughter of a U.S. Air Force Master Sergeant and a high school English teacher. She was a member of the University of Florida Law Review and published a case note on the Florida Privacy Amendment. She practiced land use and environmental law for several years but felt called to serve our veteran population and changed her practice area to veterans disability law.
Written by