“I have chronic asthma, and I use two inhalers to manage my asthma. How much will the VA rate me for my asthma?” This is a common enough question. The VA rates lung and airway conditions from 10% to 100% under the Schedule of Ratings for the Respiratory System (38 C.F.R. § 4.97). There are many kinds of respiratory conditions, and the severity can vary so greatly, that the VA most often uses pulmonary function tests (PFTs) as a basis for its rating criteria. Here’s what former military service members should know about pulmonary function tests and VA disability benefits for respiratory disorders.
Types of Respiratory Disorders
Pulmonary function disorders are grouped into two main categories: obstructive and restrictive. Putting it simply, if the air flow is impeded, the defect is obstructive. If the volume of air is reduced, the defect is restrictive. Most respiratory disorders are grouped under one of these two categories. However, there are several respiratory disorders that do not fall under either of these categories, such as:
- Tuberculosis
- Pulmonary vascular disease
- Bacterial infections of the lungs
- Mycotic lung diseases (fungal)
- Sleep apnea
Obstructive Disorders
Obstructive disorders make it difficult to exhale all the air in the lungs. Damage to the lungs, or narrowing of the airways (bronchii) inside the lungs, cause air to be exhaled more slowly than normal. This is due to reduced elasticity of the lung airways, or some kind of obstruction (like mucus or inflammation).
Obstructive lung diseases make it more difficult to breath, especially with increased activity of exertion. As the rate of breathing increases, there is less time to breathe out all the air before the next inhalation. Common obstructive disorders include:
- Chronic Obstructive Pulmonary Disease (COPD), including emphysema and chronic bronchitis
- Asthma
- Bronchiectasis
- Cystic Fibrosis
Restrictive Disorders
Restrictive disorders make it difficult to fill lungs with air. This type of lung condition is a result of the lungs being restricted from fully expanding. Usually restrictive diseases occur when there is stiffness in the lungs themselves. Sometimes this can occur when there is stiffness in the chest wall, weak muscles or damaged nerves that restrict the expansion of the lungs.
In some cases (interstitial lung diseases), autoimmune or rheumatologic diseases can cause progressive scarring of the lung tissue that lies in between and supports air sacs. Common restrictive disorders include:
- Interstitial lung disease (such as pneumonia)
- Sarcoidosis
- Asbestosis
- Pulmonary fibrosis
- Pleuritis
- Neuromuscular diseases like amyotrophic lateral sclerosis (ALS)
Dyspnea and VA Ratings for Shortness of Breath
Dyspnea, or shortness of breath, is a symptom that appears across nearly all respiratory conditions. It is not rated separately but is used to determine the severity of an underlying diagnosis. The VA will consider:
- Your PFT results (e.g., FEV-1, FEV-1/FVC, DLCO)
- Your need for medications or oxygen therapy
- Functional limitations like reduced exertion capacity
- Whether symptoms like dyspnea interfere with daily living or employment
If you experience dyspnea but your PFTs are normal, you may still be rated based on:
- Your medication regimen (e.g., daily corticosteroids)
- Need for intermittent or continuous oxygen
- DBQ documentation that clearly describes the impact of shortness of breath on your life
VA Disability Pulmonary Function Tests
A pulmonary function test (PFT) measures how much air can be inhaled and exhaled, and how much carbon monoxide can enter the bloodstream within a certain period of time. PFTs are non-invasive. A veterans doctor typically performs a pulmonary function test when initially diagnosing the condition, and then periodically afterwards to gauge the severity of the condition.
PFTs can determine whether an obstructive or restrictive disease is present, and also determine the location of a defect. A pulmonary function test measures three aspects of lung function:
- Spirometry: Measures how much and how quickly you can exhale
- Lung Volumes: Total lung capacity and how much air remains after exhaling
- DLCO: Measures how well oxygen passes from lungs to blood (important for restrictive diseases)
These measurements show how effectively you’re able to breathe and how well your lungs are able to deliver oxygen throughout the body.
How Spirometry Tests Work
The most common form of pulmonary function tests is spirometry. Spirometry is the easiest, fastest, and most readily available method of function testing in outpatient clinics. The VA rating system depends mostly on spirometry results when evaluating a respiratory disorder.
A spirometer is a hand-held device into which the individual breathes. Usually a clip is placed on the nose to prevent any air from entering the nasal passages. The patient takes a deep breath, and then exhales as hard as he/she can for at least 6 seconds (10 seconds being ideal). A small machine records the strength of the exhalation.
Because the validity of the test depends on the participation of the patient, the test is repeated two to three times in order to obtain accurate results. A spirometer has two main functions:
- It measures the forced vital capacity (FVC), which is the amount of air that can be forcibly blown out after deep inhalation.
- It also measures the forced expiratory volume in 1 second (FEV1), which is the amount of air that is forcibly blown out in the first second of the exhale. When expressed as a percentage of the “normal” averages, the FEV1 determines the degree of obstruction (if any) of the air through the lungs – mild, moderate or severe.
The VA uses post-bronchodilator results, unless they are worse than pre-bronchodilator values (in that case it chooses the pre-bronchodilator results). In other words, the least severe valid measurement is used for rating purposes.
How correct breathing affects the test
The participation of the patient is incredibly important for spirometer testing. It is a natural reaction to be hesitant about taking as deep a breath as possible or exhaling as hard as possible when taking the test. The assumption can be that the weaker the breath, the more accurate the test will be. However, this is not the case.
If the patient does not inhale deeply enough, the FVC and FEV1 will be underestimated, and the test results may mimic a restrictive disorder (such as pleural effusion or fibrosis). If the patient does not exhale hard enough, the FEV1 may be underestimated, and the result may mimic airways obstruction (such as a false positive for COPD or asthma).
In order to ensure that spirometry test results are interpreted in an accurate diagnosis, it is imperative that the patient inhale as deeply as possible, and then exhale as hard as possible for at least six seconds.
What Can I Expect from Pulmonary Function Tests?
Your doctor will provide specific instructions to prepare for your pulmonary function test. This will likely include avoiding alcohol, smoking, caffeine, and heavy exercise within the hours leading up to the test. You should also have a light meal and limit fluid intake. Be sure to wear loose clothes so you can breathe comfortably. Once you arrive at your appointment, your healthcare provider will talk you through the steps of the test.
What Should I Be Looking for in My PFT Results?
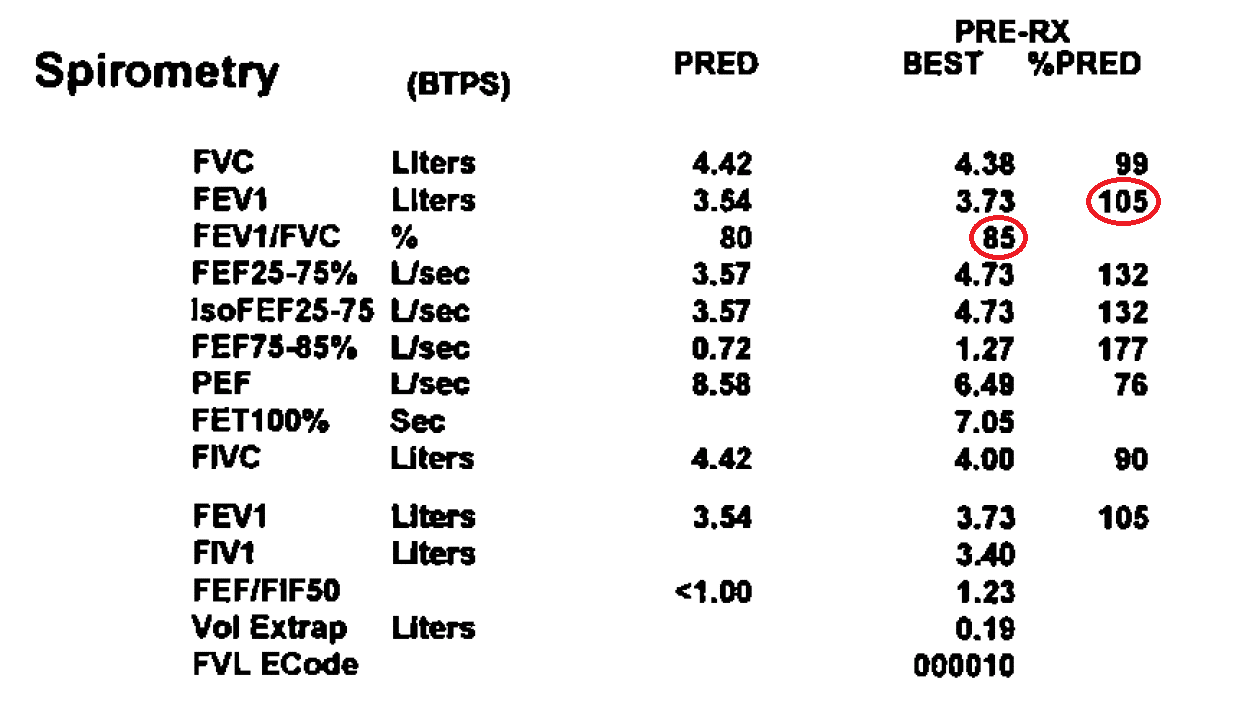
Once you have completed pulmonary function testing, your results should be available to review. However, they will be difficult for you to understand without a medical professional to interpret them for you. Spirometry results commonly look like the example below:
How the VA Rates Respiratory Disorders
VA disability ratings for respiratory conditions span from 0% to 100%, depending on the specific diagnosis, severity, treatment, and pulmonary function test (PFT) results. Once the VA determines service connection for the respiratory disorder, they will rate it on a scale based on the corresponding diagnostic code.
The VA rating schedule for respiratory disorders chiefly utilizes the numbers circled in the above example of a spirometry test. The last three columns in the image above are the ones that we are concerned with.
Example of Respiratory Disability Ratings
Think of your lungs and everything connected to them: the pipes (bronchi and trachea), the voice box (larynx), and more. A medical examiner will use a chart to figure out how severe your condition is and what kind of compensation you should get. Let’s take bronchial asthma as an example.
- 100% Rating: Your lungs are severely affected.
- Your airflow (how fast you can breathe out) is less than 40% of what it should be.
- You’re facing severe asthma attacks more than once a week.
- You need strong daily meds (like high-dose corticosteroids) to manage.
- 60% Rating: Your asthma’s bad, but not the worst.
- Your airflow is 40-55% of normal.
- You need to see the doc regularly for flare-ups.
- You’re on strong meds three or more times a year.
- 30% Rating: Your asthma’s there, but it’s under control most days.
- Your airflow is 56-70% of normal.
- You’re using inhalers or meds daily to keep things steady.
- 10% Rating: Your asthma’s mild.
- Your airflow is 71-80% of normal.
- You only need inhalers or meds every now and then.
Now, let’s really simplify the 10% rating using an example. Your doctor might give you numbers like FEV-1 or FEV-1/FVC after some breathing tests. These are just fancy ways of measuring how much and how fast you can breathe out. Let’s say, in your test:
- Line 2, Column 5 reads “105”. To get a 10% rating, this number should be between 71 and 80.
- Line 3, Column 4 reads “85”. To fit the 10% rating, this number should also be between 71 and 80.
From these two results, you wouldn’t qualify for a 10% rating. But, if you occasionally use an inhaler, then you would still fit into the 10% category (while the daily use of inhalational bronchodilators would support a 30% rating).
Remember, these ratings are all about understanding how your respiratory condition affects your life. Talk to your doctor, understand your numbers, and make sure you’re getting the support and benefits you deserve.
My Test Results Were Normal, But I Still Have Problems Breathing
Sometimes, veterans experience dyspnea or asthma attacks even when test results seem normal. How is this possible? Asthma is considered a reversible obstructive defect. This means that the use of a bronchodilator (such as albuterol) can usually open up the airways and make it easier to breathe. Most people can breathe fairly well unless they are having an active asthma attack.
Therefore, when a diagnosis of asthma is suspected, the patient will be asked to participate in other tests that can more accurately pinpoint the problem (e.g., methacholine challenge, DLCO). The VA may also rely on medication history and physician statements and consider DBQ findings on shortness of breath and activity limitations.
What Happens If My Pulmonary Function Tests Are Outdated?
Some doctors may not require regular or extensive pulmonary function tests. This can be a problem in terms of VA claims, since most of the rating schedules for respiratory disorders depend heavily on pulmonary function testing.
An outdated test will likely not be an accurate representation of the respiratory condition. A similar problem exists in cases in which spirometry results indicate little or no respiratory dysfunction.
More advanced methods of pulmonary function testing, such as the measurement of lung volumes and diffusion capacity, may not be readily accessible in outpatient clinics and therefore not available the VA examiner’s review.
However, in the event that pulmonary function testing is not available or reflective the veteran’s actual condition, the VA offers another point of reference in the rating criteria: the use of medications for management of the condition.
Specifically, the rating criteria identify the use of corticosteroids (inhaled or oral), as in asthma cases, or the use of oxygen therapy, antibiotics, and immunosuppressives as reference points for the severity of the condition.
For example, if a veteran with asthma requires daily use of a bronchodilator inhaler to manage his asthma, he would be entitled to a 30% rating.
Whichever the case may be, the VA tries its best to cover every possible situation by the thoroughness of its Disability Benefits Questionnaire (DBQ) for respiratory disorders.
On examination of the patient, VA examiners are requested to indicate whether or not pulmonary function testing was performed, and if the testing accurately reflected the actual state of the veteran’s respiratory condition. The DBQ devotes a section for use of medications, bronchodilators, corticosteroids, antibiotics, and oxygen therapy that the veteran may be prescribed for the management of the respiratory disorder.
This questionnaire can also be completed by the veteran’s treating physician, as additional evidence in support of the veteran’s claim in the event that the C&P examiner was not sufficiently thorough or accurate.
Use your DBQ, track your PFT results, and don’t hesitate to have your private physician complete a DBQ to supplement your claim. Even if your numbers look normal, your symptoms may still warrant compensation. The more complete your evidence, the better the VA can understand the true impact of your respiratory condition.
What If I Can’t Work Because of My Respiratory Issues?
Total Disability Based on Individual Unemployability is a VA benefit that allows veterans to be compensated at the 100% disability rate, even if their rating is less than 100%, when their disabilities make employment unsustainable or impossible. Veterans with respiratory disorders may qualify for TDIU if these conditions (alone or combined with others):
- Severely limit physical exertion
- Cause dyspnea (shortness of breath) on minimal activity
- Require continuous oxygen therapy
- Lead to frequent medical treatment or hospitalizations
- Interfere with concentration, stamina, or endurance, especially in physically demanding or even sedentary jobs
Pathways to TDIU
Schedular TDIU
- You have one service-connected condition rated at 60% or more, OR
- You have two or more conditions, with one rated at least 40%, and a combined rating of 70% or more
Examples: A veteran with COPD rated at 60% who cannot perform any physical labor due to shortness of breath.
Extraschedular TDIU
If you do not meet the percentage thresholds, but your respiratory condition still prevents you from working, the VA must refer your claim to the Director of Compensation Service for consideration.
Example: A veteran rated at 30% for asthma and 30% for sleep apnea, with constant fatigue and dyspnea that make working impossible.
These claims are often under-supported, so it’s vital to document how the condition limits physical or sedentary work, treatment demands (e.g., oxygen, steroids, hospital visits) and the real-world impact on day-to-day functioning. Our TDIU lawyers can assist you in getting full benefits for your breathing impairment.

Written by